

Pharmacokinetic bioequivalence of semaglutide injection in healthy adults under fasting conditions: A randomized study

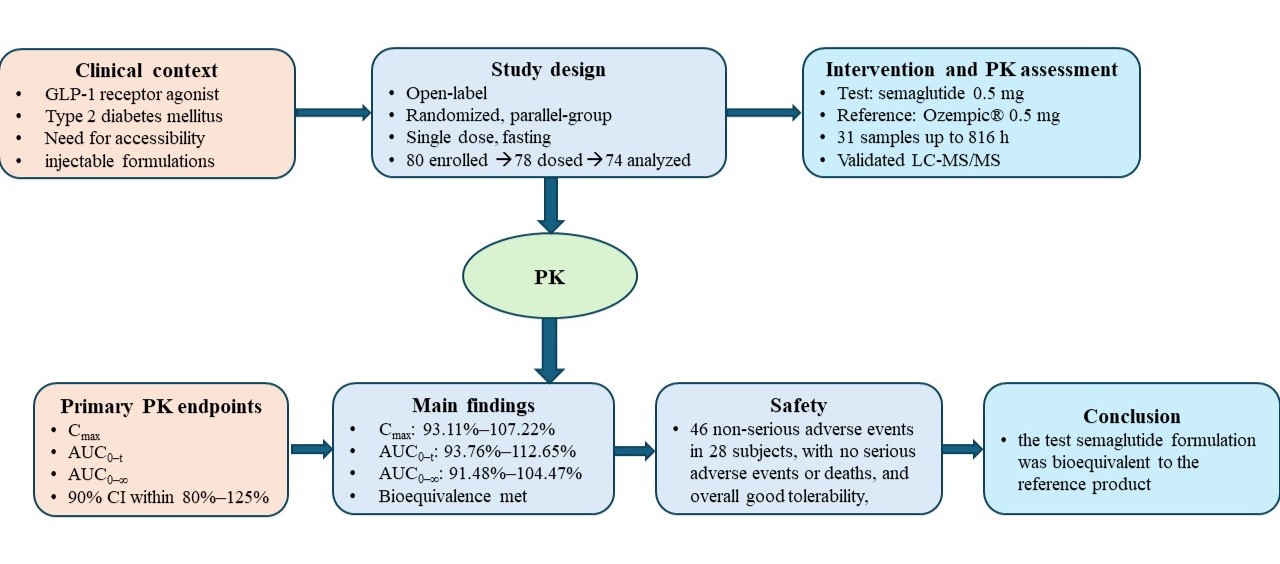
Background: Semaglutide is a long-acting glucagon-like peptide-1 receptor agonist used in the management of type 2 diabetes mellitus. Broader access to semaglutide therapy may be supported by clinically suitable alternative formulations if pharmacokinetic comparability with the reference product is established. Aim: To evaluate the pharmacokinetic bioequivalence of semaglutide 0.5 mg solution for injection developed by Dr. Reddy’s Laboratories Limited, India, compared with Ozempic® (semaglutide) 0.5 mg solution for injection in a pre-filled pen under fasting conditions in healthy adult subjects. Methods: This was an open-label, balanced, randomized, two-treatment, single-dose, parallel-group bioequivalence study. Eighty healthy volunteers were enrolled, 78 were dosed, and 74 were included in the pharmacokinetic and statistical analyses. Plasma semaglutide concentrations were measured using a validated liquid chromatography–tandem mass spectrometry method across 31 sampling time points up to 816 hours after dosing. Primary pharmacokinetic endpoints were Cmax, area under the curve (AUC)0–t, and AUC0–∞. Bioequivalence was concluded if the 90% confidence intervals for the test/reference ratio were within 80% to 125%. Results: The 90% confidence intervals were 93.11%–107.22% for Cmax, 93.76%–112.65% for AUC0–t, and 91.48%–104.47% for AUC0–∞, meeting bioequivalence criteria for all primary parameters. Forty-six non-serious adverse events were reported in 28 subjects. No serious adverse events or deaths occurred. Conclusion: The test semaglutide formulation was bioequivalent to the reference product and was generally well tolerated in healthy adult subjects under fasting conditions. Relevance for patients: A pharmacokinetically comparable semaglutide injection may help expand access to long-term semaglutide treatment where innovator product cost or availability may limit patient use.
- Bajaj M, McCoy RG, Balapattabi K, et al. Summary of Revisions: Standards of Care in Diabetes—2026. Diabetes Care. 2025;49(Supplement_1):S6-S13. doi: 10.2337/dc26-srev
- Yang XD, Yang YY. Clinical pharmacokinetics of semaglutide: a systematic review. Drug Des Devel Ther. 2024;18:2555-2570. doi: 10.2147/DDDT.S470826
- Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev. 2007;87(4):1409-1439. doi: 10.1152/physrev.00034.2006
- Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740-756. doi: 10.1016/j.cmet.2018.03.001
- Nauck MA, Meier JJ. Management of endocrine disease: are all GLP-1 receptor agonists equal in the treatment of type 2 diabetes? Eur J Endocrinol. 2019;181(6):R211-R234. doi: 10.1530/EJE-19-0566
- Lau J, Bloch P, Schäffer L, et al. Discovery of the once-weekly glucagon-like peptide-1 analogue semaglutide. J Med Chem. 2015;58(18):7370-7380. doi: 10.1021/acs.jmedchem.5b00726
- Jensen L, Helleberg H, Roffel A, et al. Absorption, metabolism and excretion of the GLP-1 analogue semaglutide in humans and nonclinical species. Eur J Pharm Sci. 2017;104:31-41. doi: 10.1016/j.ejps.2017.03.020
- Knudsen LB, Lau J. The discovery and development of liraglutide and semaglutide. Front Endocrinol. 2019;10:155. doi: 10.3389/fendo.2019.00155
- Granhall C, Donsmark M, Blicher TM, et al. Safety and pharmacokinetics of single and multiple ascending doses of the novel oral human GLP-1 analogue, oral semaglutide, in healthy subjects and subjects with type 2 diabetes. Clin Pharmacokinet. 2019;58(6):781-791. doi: 10.1007/s40262-018-0728-4
- Kapitza C, Nosek L, Jensen L, Hartvig H, Jensen CB, Flint A. Semaglutide, a once-weekly human GLP-1 analog, does not reduce the bioavailability of the combined oral contraceptive ethinylestradiol/levonorgestrel. J Clin Pharmacol. 2015;55(5):497-504. doi: 10.1002/jcph.443
- Bækdal TA, Breitschaft A, Donsmark M, Maarbjerg SJ, Søndergaard FL, Borregaard J. Effect of various dosing conditions on the pharmacokinetics of oral semaglutide, a human glucagon-like peptide-1 analogue in a tablet formulation. Diabetes Ther. 2021;12(7):1915-1927. doi: 10.1007/s13300-021-01078-y
- Petri KCC, Ingwersen SH, Flint A, Zacho J, Overgaard RV. Exposure-response analysis for evaluation of semaglutide dose levels in type 2 diabetes. Diabetes Obes Metab. 2018;20(9):2238-2245. doi: 10.1111/dom.13358
- Overgaard RV, Navarria A, Ingwersen SH, Bækdal TA, Kildemoes RJ. Clinical pharmacokinetics of oral semaglutide: analyses of data from clinical pharmacology trials. Clin Pharmacokinet. 2021;60(10):1335-1348. doi: 10.1007/s40262-021-01025-x
- Sorli C, Harashima SI, Tsoukas GM, et al. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017;5(4):251-260. doi: 10.1016/S2213-8587(17)30013-X
- Ahrén B, Masmiquel L, Kumar H, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes: SUSTAIN 2. Lancet Diabetes Endocrinol. 2017;5(5):341-354. doi: 10.1016/S2213-8587(17)30092-X
- Ahmann AJ, Capehorn M, Charpentier G, et al. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes: SUSTAIN 3. Diabetes Care. 2018;41(2):258-266. doi: 10.2337/dc17-0417
- Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin with or without sulfonylureas in insulin-naive patients with type 2 diabetes: SUSTAIN 4. Lancet Diabetes Endocrinol. 2017;5(5):355-366. doi: 10.1016/S2213-8587(17)30085-2
- Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes: SUSTAIN 5. J Clin Endocrinol Metab. 2018;103(6):2291-2301. doi: 10.1210/jc.2018-00070
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. doi: 10.1056/NEJMoa1607141
- Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes: SUSTAIN 7. Lancet Diabetes Endocrinol. 2018;6(4):275-286. doi: 10.1016/S2213-8587(18)30024-X
- Lingvay I, Catarig AM, Frias JP, et al. Efficacy and safety of once-weekly semaglutide versus daily canagliflozin as add-on to metformin in patients with type 2 diabetes: SUSTAIN 8. Lancet Diabetes Endocrinol. 2019;7(11):834- 844. doi: 10.1016/S2213-8587(19)30311-0
- Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109-121. doi: 10.1056/NEJMoa2403347
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183
- Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/s0140-6736(21)00213-0
- Aroda VR, Rosenstock J, Terauchi Y, et al. PIONEER 1: randomized clinical trial of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care. 2019;42(9):1724-1732. doi: 10.2337/dc19-0749
- Rosenstock J, Allison D, Birkenfeld AL, et al. Effect of additional oral semaglutide vs sitagliptin on glycated hemoglobin in adults with type 2 diabetes uncontrolled with metformin alone or with sulfonylurea: PIONEER 3. JAMA. 2019;321(15):1466-1480. doi: 10.1001/jama.2019.2942
- Nielsen MS, Brøndsted L, Kankam M, Morelli G, Nguyen D, Skjøth TV, et al. A bioequivalence study of two formulations of oral semaglutide in healthy participants. Diabetes Ther. 2025;16(2):269-287. doi: 10.1007/s13300-024-01674-8
- Bouhajib M, Tayab Z, Di Marco C, Suh D. The pharmacokinetics and comparative bioavailability of oral and subcutaneous semaglutide in healthy volunteers. J Basic Clin Physiol Pharmacol. 2025;36(2-3):221-227. doi: 10.1515/jbcpp-2025-0026
- Mayabhate MM, Kapure N, Sharma A, Vaddem R. Bridging Innovation and Access: Randomized, Single-Dose, Open- Label, Parallel-Group Bioequivalence Study of Generic and Innovator Injection Semaglutide in India. Am J Pharmacol Toxicol. 2026;20(1):9-15. doi: 10.3844/ajptsp.2026.9.15
- Mendis S, Fukino K, Cameron A, et al. The availability and affordability of selected essential medicines for chronic diseases in six low- and middle-income countries. Bull World Health Organ. 2007;85(4):279-288. doi: 10.2471/BLT.06.033647
- Alatorre C, Fernández Landó L, Yu M, et al. Treatment patterns in patients with type 2 diabetes mellitus treated with glucagon-like peptide-1 receptor agonists: higher adherence and persistence with dulaglutide compared with once-weekly exenatide and liraglutide. Diabetes Obes Metab. 2017;19(7):953-961. doi: 10.1111/dom.12902
- European Medicines Agency. Guideline on the Investigation of Bioequivalence. CPMP/EWP/QWP/1401/98 Rev. 1/ Corr**. 2010. Accessed July 1, 2026. https://www.ema.europa.eu/en/investigation-bioequivalence-scientific-guideline
- US Food and Drug Administration. Statistical approaches to establishing bioequivalence: guidance for industry. 2026. Accessed July 1, 2026. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/statistical-approaches-establishing-bioequivalence
- US Food and Drug Administration. Bioavailability studies submitted in NDAs or INDs—general considerations: guidance for industry. 2022. Accessed July 1, 2026. https://www.fda.gov/media/121311/download
- Schuirmann DJ. A comparison of the two one-sided tests procedure and the power approach for assessing bioequivalence. J Pharmacokinet Biopharm. 1987;15(6):657- 680. doi: 10.1007/BF01068419
- Agência Nacional de Vigilância Sanitária. RDC No. 742 of 10 August 2022: provides for the criteria to conduct relative bioavailability/bioequivalence studies and pharmacokinetic studies. 2022. Accessed July 1, 2026. https://www.gov.br/ anvisa/en/rules-and-regulations/arquivos/rdc-742-2022-e.pdf
- International Council for Harmonisation. ICH E6(R3): Guideline for Good Clinical Practice. 2025. Accessed July 1, 2026. https://database.ich.org/sites/default/files/ICH_E6%28R3%29_Step4_FinalGuideline_2025_0106.pdf
- Indian Council of Medical Research. National Ethical Guidelines for Biomedical and Health Research Involving Human Participants. 2017. Accessed July 1, 2026. https://www.icmr.gov.in/icmrobject/custom_data/pdf/resource-guidelines/ICMR_Ethical_Guidelines_2017.pdf
- World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human participants. JAMA. 2025;333(1):71-74. doi: 10.1001/jama.2024.21972
- International Council for Harmonisation. ICH M10: Bioanalytical Method Validation and Study Sample Analysis. 2022. Accessed July 1, 2026. https://database.ich.org/sites/default/files/M10_Guideline_Step4_2022_0524.pdf
- US Food and Drug Administration. M10 Bioanalytical Method Validation and Study Sample Analysis: Guidance for Industry. 2022. Accessed July 1, 2026. https://www.fda.gov/ regulatory-information/search-fda-guidance-documents/m10-bioanalytical-method-validation-and-study-sample-analysis
- Viswanathan CT, Bansal S, Booth B, et al. Quantitative bioanalytical methods validation and implementation: best practices for chromatographic and ligand binding assays. AAPS J. 2007;9(1):E30-E42. doi: 10.1208/aapsj0901004
- Bansal S, DeStefano A. Key elements of bioanalytical method validation for small molecules. AAPS J. 2007;9(1):E109-E114. doi: 10.1208/aapsj0901011
- DeSilva B, Smith W, Weiner R, et al. Recommendations for the bioanalytical method validation of ligand-binding assays to support pharmacokinetic assessments of macromolecules. Pharm Res. 2003;20(11):1885-1900. doi: 10.1023/B:PHAM.0000003390.51761.3d